










Tongue-tie should be diagnosed based on physical abnormality AND functional need. Looking at a picture of a tongue does not offer information about how successful the child is in feeding or speaking. Some practitioners use location of restriction to determine severity or class of tie, but ultimately it should always be based on the primary concerns and functional ability.
Although newborns are screened for a variety of abnormalities during the routine birth assessment, this often does not include assessment for tongue-tie. Unfortunately, it is highly unlikely a generalized pediatrician or nurse will have specific training in tongue-tie assessment and therefore will miss the restriction or incorrectly diagnose. Although it is not typically routine for every birth, most hospitals can offer certified lactation consultants when requested.
Preferred providers for tongue-tie include the following who have specifically gained specialized training and education beyond their general practice: pediatric dentists, ENTs, international board-certified lactation consultants (IBCLC), speech-language pathologists (SLP), and oromyofacial therapists.
When a tongue-tie is suspected, a referral to a specialized preferred provider both skilled and knowledgeable in feeding and tongue-tie is essential. The assessment should include a thorough birth and breastfeeding/feeding history with present concerns highlighted (functional needs). The professional should also observe a feeding if at all possible and assess suck and tongue function. This typically involves putting a finger in the child’s mouth to evaluate how the infant uses their tongue to coordinate suck, swallow, and breathe patterns necessary for feeding. Additionally, the tongue is assessed for range of motion or how the tongue moves side to side and up and down.
Correct examination of infants requires the infant to be placed on the examiner’s lap with the infant’s head facing the same direction as the person evaluating and the infant’s feet in the caregiver’s lap. Assessment in a different position will likely lead to an incorrect or missed diagnosis.

A recommended treatment plan could involve the following steps:
- Assessment of feeding and functional concerns and treatment trial if necessary.
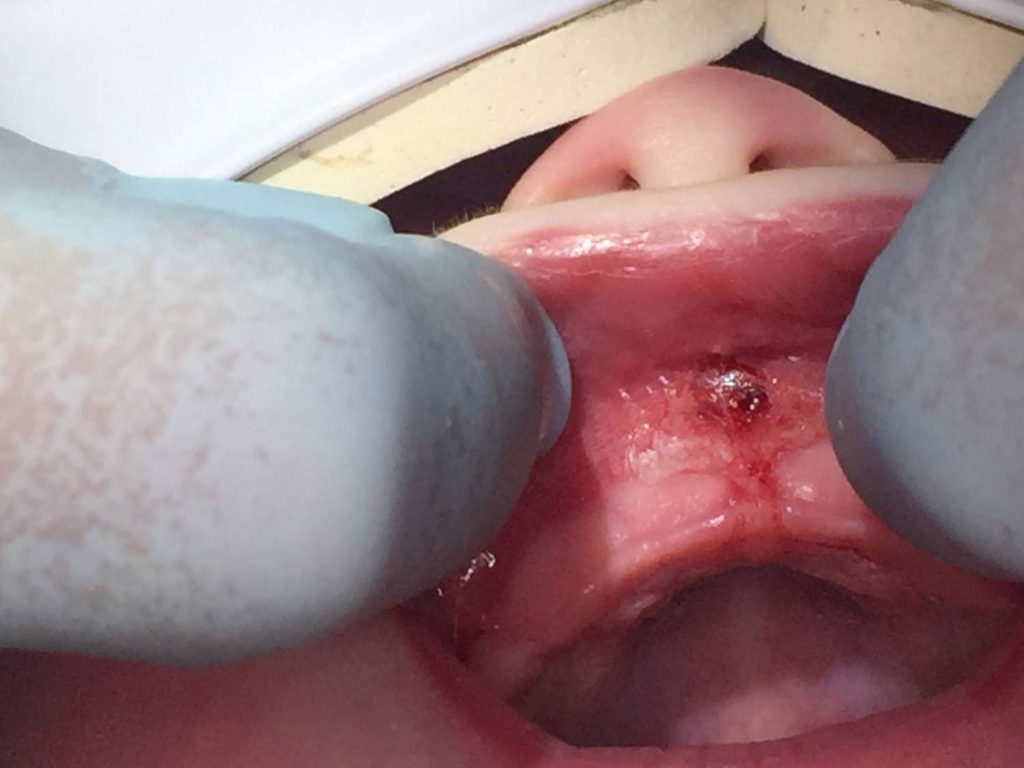
- Tongue-tie release by practitioner resulting in diamond-shaped cut
- Wound management by caregiver
- Feeding therapy (speech-language pathologist) or lactation support, if needed
- Other therapy as needed, such as Oral Myofunctional Therapy, physical therapy, occupational therapy, chiropractic, Cranial Sacral Therapy, Osteopathic Manipulative Therapy, or massage therapy.
Tongue-tie release, known as a frenotomy or frenectomy, is a small incision into the connective tissue to allow more movement of the tongue, lips, and/or cheeks. The practitioner may use sterile scissors or water laser to clip or release the restricted tissue to allow for more range of motion.
This procedure is typically done in an office setting with only local analgesia or nothing at all. There is very little risk and usually very effective in improving function with follow-up care and supportive therapy. Talk with your preferred provider to learn more about which method they use for release. Most preferred providers now use a laser frenectomy, as it is quick and effective, has a lower risk of infection, reduced post-surgical pain and swelling.
Uncommon risks of tongue-tie release procedure include:
- Recurrence – most common complication due to improper post-operative wound management (stretches/exercise) or inefficient release the first time
- Minor bleeding
- Infection
- Pain
- Damage to tongue and salivary ducts in the mouth
A tongue-tie release is the act of cutting the tissue as needed for functional movement.
Tongue-tie revision is when a secondary release is required due to reattachment or lack of complete release.
The mouth heals relatively quickly in comparison to other parts of the body. Also, open oral wounds contract towards the center as it is healing. However, in order for the tissue not to reattach, we need to slow the healing process and keep the wound open in order for the wound to heal from the inside first. Your preferred provider will provide specific instructions for exercises and care following the procedure. It may include stretching the area, massaging the wound, or moving the tongue. These stretches are typically recommended for 2-3 weeks following the procedure.
More information on what to expect with wound management.
Some people report they see immediate results after the tongue-tie release, but for others it may take up to 2-3 weeks to re-learn swallowing motor patterns. However, if wound management is not successful and tongue reattaches, results will naturally take longer.
Imagine, as a runner, you had to run every race with your shoes tied together. You could probably finish the race eventually, but it wouldn’t be very graceful. Then on day, you untie the knot and now are able to run without restriction, but you’ve never ran like this before. You need to re-learn how to run in this new way. It takes time and effort to re-learn, but eventually you are able to run gracefully and finish the race faster.
This is how it feels to have a tongue-tie release. The child likely has learned maladaptive compensatory strategies to overcome the restriction. After the tongue is released, the muscles do not have the patterns established for free movement and must learn new patterns for eating and speaking. Now that there is no abnormal tissue tethering the tongue, it may even rest in a new position in the mouth during breathing and sleeping.
Therapy can be extremely beneficial to helping establish these new patterns as well as assist in wound care immediately following the procedure to ensure reattachment does not happen.
This is why therapy is so important. The child has learned to compensate with a restricted tongue and now has full range of motion, but isn’t practiced in using it. It can take a few weeks for the child to learn how to use their tongue during feeding.
No, this is not true. Even in utero, a baby learns to swallow. After birth, we swallow between 500-700 times a day. If our tongue is restricted and unable to swallow correctly, we will learn to use compensatory strategies. The habit of incorrect swallowing pattern is reinforced and may contribute to atypical development and issues later in life.
No, weight gain is not the only sign of a successful feeding relationship. If you have concerns or see any of the red flags listed above, you should seek a tongue-tie assessment from a preferred provider.
International Association of Tongue-Tie Professionals (IATP) -FAQs and research
Dr. Lawrence Kotlow, DDS -research and articles
Dr. Bobby Ghaheri, MD -research and articles
Alabama Tongue-Tie Center -videos
Tongue-Tie Book – free download
I just found your website. I am a general dentist of 40+ years, have been treating TOTS since 1984.
Your site is excellent! Very informative. May I refer by patients to it?
Yes, of course. Thank you!
It helped when you wrote that tongue-tie is more common among boys. My friend wants to treat her child’s tongue tie. I think it’s best for her to look for a dental clinic that specializes in tongue releases.
Definitely tell her to have a doctor trained in it and not do it herself. Youe mouth is full of germs . All I have to do is suck my finger if I have pulled a hangnail off and it’s bleeding and it gets infected.
I never took into account the fact that untreated tongue tie issues can also affect the sleep, dental, oral, facial, speech, and other aspects of an individual. So it’s important that my sister immediately gets her daughter diagnosed to see if her daughter needs to undergo tongue-tie surgery. Because we all noticed that there is something different with how her daughter eats or makes sounds as a baby.
Your information is very helpful. It is very frustrating that for most families, the procedure and follow up is not covered by insurance.